
Low Level Laser Therapy
Harnessing visible light photons to elevate electrons for innovative chemical reactions in health applications.
The realm of laser therapy can be a labyrinth of bewildering terminology, often diverging from its conventional meanings. This confusion stems from a lack of comprehension among many companies, who merely echo past statements without genuine understanding. Yet, amidst this perplexity, Erchonia® stands as a beacon of clarity and commitment.
If you’ve encountered the name Erchonia®, we hope one consistent theme would resonate: our unyielding dedication to comprehending laser therapy through the most stringent clinical research standards and our steadfast faith in low-level laser therapy. Unlike conventional enterprises, Erchonia® wasn’t born from a calculated marketing strategy to peddle a product. Instead, it arose from an imperative—to further explore and develop a technology that alleviated our founder’s father from pain. Our mission remains rooted in spreading this transformative technology far and wide, aiding those grappling with similar afflictions, and enlightening healthcare providers on the significance of low-level lasers.
At Erchonia®, we recognize this pervasive confusion and are committed to illuminating the path forward. The distinction between “Power” and “Energy” in laser therapy serves as a prime example of this complexity. While these terms are often used interchangeably, their meanings carry distinct significance, influencing the effectiveness and safety of laser treatments. Let us delve deeper into this critical distinction, shedding light on its implications for practitioners and patients alike.
POWER
Ah, yes, the ubiquitous term in laser therapy discussions—power. We’ve all heard the comparisons: “100 times more powerful” or “10 times more potent.” But let’s break it down: power is essentially the number of photons a laser emits every second. Sounds impressive, right? But here’s the kicker: most of these conversations miss the mark on what power truly means and how less than crucial it is in laser therapy. To put it into perspective, imagine a laser operating at a wavelength of 630 nm and a power output of 5 mW. Now, let’s crunch some numbers to figure out how many photons this laser churns out every second. Using fundamental physics formulas, we determine that approximately 1.597×10^16 photons are emitted by the laser per second. That’s billions upon billions of photons buzzing around in just one second!
But here’s where it gets interesting: ramping up the power of a laser doesn’t necessarily mean better results. Why? Because no matter how impressive the photon count sounds, if the energy of those photons is too low to initiate the photochemical reaction, it’s all for naught. In essence, it’s not about “more power.” It’s about understanding the true essence of power in laser therapy—how it interacts with the body’s biology and quantum physics principles. After all, it only takes one photon to kickstart the photochemical reaction, rendering the notion of “more power” obsolete.
So, the next time you hear the term “power” thrown around in laser therapy discussions, remember it’s not about quantity, but quality. It’s about harnessing the right amount of energy, not power to ignite the healing process within the body—a concept that Erchonia® champions wholeheartedly.
ENERGY
Now, let’s talk about electron volts—a term that sounds like it belongs in a science fiction novel, but it’s actually a key player in the world of atomic and nuclear physics. Essentially, an electron volt (eV) is the amount of energy gained by an electron when it’s zipping through an electric potential difference—kind of like a roller coaster ride for electrons. Picture this: each electron gets a boost of energy as it accelerates from “rest” to “excited,” thanks to this electric potential difference.
But why does this matter? Well, this electrifying journey is what stimulates our cells and triggers that magical photochemical response we’re all after. In other words, it’s the spark that ignites the healing process within our bodies. So, while it may sound like something straight out of a sci-fi flick, electron volts are actually the unsung heroes of laser therapy, quietly powering the transformative effects we’ve come to rely on. And when it comes to understanding the science behind laser therapy, knowing the role of electron volts is like unlocking the secret to its success.
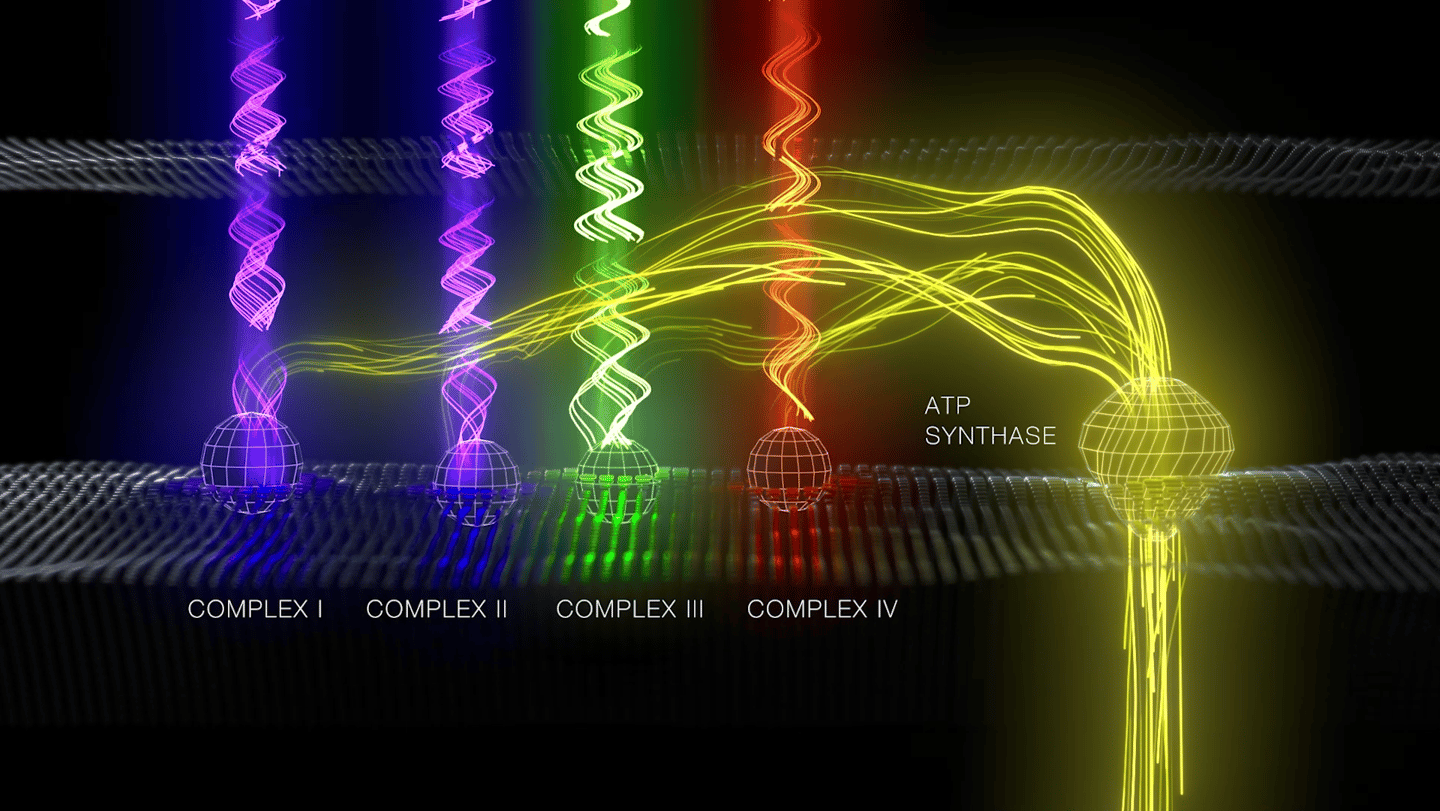
And here’s where Erchonia® steps in with a game-changer: multiple wavelength lasers. Each wavelength boasts its own unique electron volt (eV) output, and only precise matches of energy will kickstart those vital protein complexes within the mitochondria. We’re talking about the Electron Transport Chain (ETC), the powerhouse where all the magic of laser therapy unfolds. And guess what? It’s got nothing to do with power and everything to do with energy.
So, whether it’s understanding the intricate dance between wavelengths or unraveling the mysteries of electron volts, Erchonia® is committed to illuminating the path forward in laser therapy—because when it comes to healing, every detail matters.
How Laser Therapy Works.
Low-Level Laser Therapy (LLLT) works by delivering specific light wavelengths (typically red, near-infrared, or in Erchonia’s case, green and violet) to targeted tissues. These photons are absorbed by mitochondria—the cell’s “power plants”—especially cytochrome c oxidase. This stimulates increased production of adenosine triphosphate (ATP), the energy currency of the cell. With more ATP, cells repair, regenerate, and function more efficiently. LLLT also helps reduce oxidative stress, modulate inflammation, improve circulation, and promote tissue healing. Unlike high-power lasers, LLLT is non-thermal, meaning it does not burn or cut tissue, making it safe, painless, and non-invasive for therapeutic use.
Laser Classifications
Photon Absorption
Visible light photons elevate electrons, enabling crucial chemical reactions in molecules, enhancing therapeutic applications and promoting healing through advanced laser technology.
Molecular Excitement
The process of molecular excitement occurs when photons elevate electrons, facilitating energy transfer and chemical reactions essential for various applications in health and wellness.
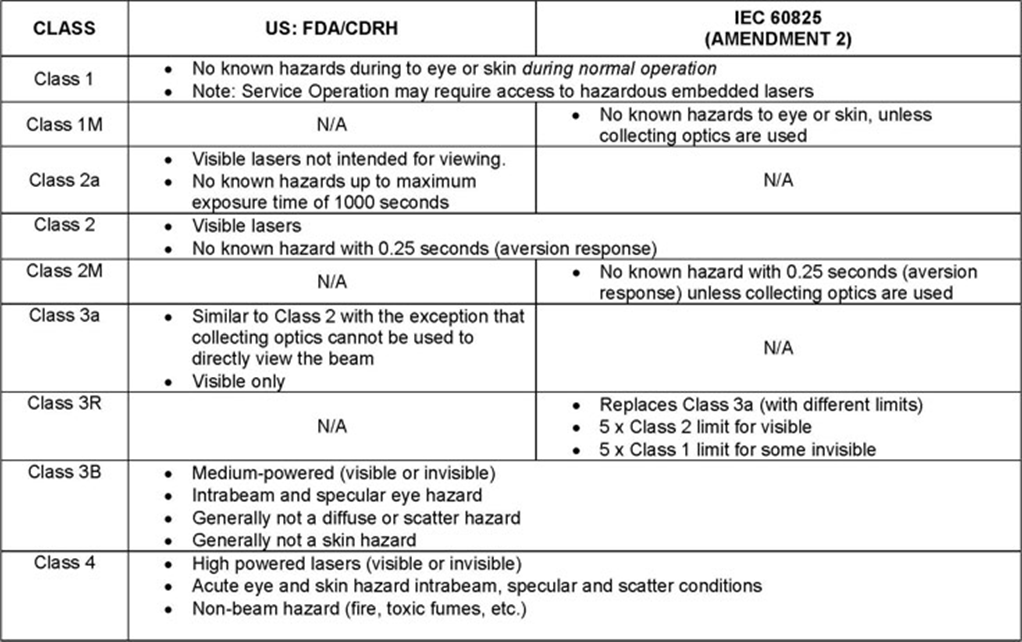
Lasers have been classified by wavelength and maximum output power into four classes and a few subclasses since the early 1970s. The classifications categorize lasers according to their ability to produce damage in exposed people, from class 1 (no hazard during normal use) to class 4 (severe hazard for eyes and skin). The classification of a laser is based on the concept of accessible emission limits (AEL) that are defined for each laser class. This is usually a maximum power (in W) or energy (in J) that can be emitted in a specified wavelength range and exposure time. For infrared wavelengths above 4 μm, it is specified as a maximum power density (in W/m2). It is the responsibility of the manufacturer to provide the correct classification of a laser, and to equip the laser with appropriate warning labels and safety measures as prescribed by the regulations. Safety measures used with the more powerful lasers include key-controlled operation, warning lights to indicate laser light emission, a beam stop or attenuator, and an electrical contact that the user can connect to an emergency stop or interlock.There are two classification systems in use, one based on the FDA laser regulations in existence prior to 2002, and one based on the international standard IEC 60825. At present the IEC 60825 laser classification system is not fully harmonized with US laser regulation, although products labeled with the IEC 60825 derived system are accepted. Since the laser devices manufactured by Erchonia are used world-wide each device is labeled under both the original US laser classification system and the IEC 60825 classification system. Below is a comparison chart depicting the classifications and the regulations that are associated with each. Following the chart is a more detailed description of each classification.
Class 1 — A class 1 laser is safe under all conditions of normal use. This means the maximum permissible exposure (MPE) cannot be exceeded. This class includes high-power lasers within an enclosure that prevents exposure to the radiation and that cannot be opened without shutting down the laser. For example, a continuous laser at 600 nm can emit up to 0.39 mW, but for shorter wavelengths, the maximum emission is lower because of the potential of those wavelengths to generate photochemical damage. The maximum emission is also related to the pulse duration in the case of pulsed lasers and the degree of spatial coherence.
Class 1M — A Class 1M laser is safe for all conditions of use except when passed through magnifying optics such as microscopes and telescopes. Class 1M lasers produce large-diameter beams, or beams that are divergent. The MPE for a Class 1M laser cannot normally be exceeded unless focusing or imaging optics are used to narrow the beam. If the beam is refocused, the hazard of Class 1M lasers may be increased and the product class may be changed. A laser can be classified as Class 1M if the total output power is below class 3B but the power that can pass through the pupil of the eye is within Class 1.
Class 2 — A Class 2 laser is safe because the blink reflex will limit the exposure to no more than 0.25 seconds. It only applies to visible-light lasers (400–700 nm). Class-2 lasers are limited to 1 mW continuous wave, or more if the emission time is less than 0.25 seconds or if the light is not spatially coherent. Intentional suppression of the blink reflex could lead to eye injury. Many laser pointers are class 2.
Class 2M — A Class 2M laser is safe because of the blink reflex if not viewed through optical instruments. As with class 1M, this applies to laser beams with a large diameter or large divergence, for which the amount of light passing through the pupil cannot exceed the limits for class 2.
Class 3R — A Class 3R laser is considered safe if handled carefully, with restricted beam viewing. With a class 3R laser, the MPE can be exceeded, but with a low risk of injury. Visible continuous lasers in Class 3R are limited to 5 mW. For other wavelengths and for pulsed lasers, other limits apply.
Class 3B — A Class 3B laser is hazardous if the eye is exposed directly, but diffuse reflections such as from paper or other matte surfaces are not harmful. Continuous lasers in the wavelength range from 315 nm to far infrared are limited to 0.5 W. For pulsed lasers between 400 and 700 nm, the limit is 30 mJ. Other limits apply to other wavelengths and to ultrashort pulsed lasers. Protective eyewear is typically required where direct viewing of a class 3B laser beam may occur. Class-3B lasers must be equipped with a key switch and a safety interlock.
Class 4 — Class 4 lasers include all lasers with beam power greater than class 3B. By definition, a class-4 laser can burn the skin, in addition to potentially devastating and permanent eye damage as a result of direct or diffuse beam viewing. These lasers may ignite combustible materials, and thus may represent a fire risk. Class 4 lasers must be equipped with a key switch and a safety interlock. Many industrial, scientific, military, and medical lasers are in this category.
This classification system is only slightly altered from the original system developed in the early 1970s. It is still used by US laser product safety regulations. The laser powers mentioned are typical values. Classification is also dependent on the wavelength and on whether the laser is pulsed or continuous.
Class I — Inherently safe; no possibility of eye damage. This can be either because of a low output power (in which case eye damage is impossible even after hours of exposure), or due to an enclosure preventing user access to the laser beam during normal operation, such as in CD players or laser printers.
Class II — The blink reflex of the human eye (aversion response) will prevent eye damage, unless the person deliberately stares into the beam for an extended period. Output power may be up to 1 mW. This class includes only lasers that emit visible light. Some laser pointers are in this category.
Class IIa — A region in the low-power end of Class II where the laser requires in excess of 1000 seconds of continuous viewing to produce a burn to the retina. Supermarket laser scanners are in this subclass.
Class IIIa — Lasers in this class are mostly dangerous in combination with optical instruments which change the beam diameter or power density. Output power does not exceed 5 mW. Beam power density may not exceed 2.5 mW/square cm. Many laser sights for firearms and laser pointers are in this category.
Class IIIb — Lasers in this class may cause damage if the beam enters the eye directly. This generally applies to lasers powered from 5–500 mW. Lasers in this category can cause permanent eye damage with exposures of 1/100th of a second or less depending on the strength of the laser. A diffuse reflection is generally not hazardous but specular reflections can be just as dangerous as direct exposures. Protective eyewear is recommended when direct beam viewing of Class IIIb lasers may occur. Lasers at the high power end of this class may also present a fire hazard and can lightly burn skin.
Class IV — Lasers in this class have output powers of more than 500 mW in the beam and may cause severe, permanent damage to eye or skin without being magnified by optics of eye or instrumentation. Diffuse reflections of the laser beam can be hazardous to skin or eye within the Nominal Hazard Zone. Many industrial, scientific, military, and medical lasers are in this category.
WriteThe Power and Penetration Myth
Erchonia Corporation
Low Level Laser Therapy: The Power and Penetration Myth: The understanding of how the human body functions in conjunction with low level laser therapy (LLLT, 3LT®, cold laser) is an advancing paradigm in modern wellness approaches. These transformative changes are encouraging a clearer understanding of the mechanism of how each new invention affects each system. 3LT® is not excluded from the advancing medical technology that requires continual scientific evidence of the mechanism before we can thoroughly comprehend the magnitude of the neurological and physiological changes taking place. Nevertheless, 3LT® is one of the few devices that have published, peer-reviewed double blinded controlled studies dating back over twenty years and many “clinicians and researchers are unaware of the extensive research that has been done in field of biophysics, bionics, photobiology and quantum biology during the past eighty years”1 that aid in clarity of the mechanism of laser applications. The first milestone made in the United States for 3LT® was a FDA approval in 2002. With this approval came a new classification of therapeutic devices, referred to as NHN,2 which is a category for non-heating modalities for adjunctive use in pain therapy commonly known as biostimulation, which we will address later. The first market clearance (510k approval) was issued for the treatment of neck and shoulder pain. Since this accomplishment, the FDA has issued 510(k) clearances in the NHN category for the treatment of carpal tunnel and post surgical pain based on clinical data and cellular/molecular research. Unfortunately, other laser companies have not adhered to such standards of their therapeutic devices and have filed what is referred to as ‘substantial equivalence’ against a laser previously granted market clearance by acceptable completion of clinical trial data. A ‘substantial equivalence’ submission to the FDA is authored by the company or a representative of the company that is intending to obtain market clearance without conducting clinical trials. The substantial equivalence document shows the device attempting to obtain market clearance being compared against a device that already has been awarded market clearance by comparison of features and components. The company submitting a substantial equivalence document, using the features and components comparison as a catalyst, then authors a narrative explaining why the device they are vying for fits in the same category of therapeutic applications of the laser or laser(s) being compared to. Laser Classification is a regulated feature of a laser device and is a component of comparison in a substantial equivalence submission. As recently quoted in Tunér and Hodes’s article Confounders and magicians,3 classification of laser devices are determined by “…the possible risk for eye injuries and has nothing to do with the efficiency in treatment… The classification is not only a question of output power; it has to do with wavelength, divergence of the beam, emission area, pulsing etc.” The FDA approval process is extremely complex; this brief explanation is simply a highlight of the proceedings of receiving a laser approval and also to show that the considerations of the approval are independent of the advertising and marketing which follow. Jan. 2008 The most recent flux of laser advertising has led to a great deal of confusion pertaining to the field. Much of this confusion about the use of therapeutic lasers stems from attempting to look at laser effects from a Newtonian mechanistic perspective that has now been supplanted by non-linear dynamics and quantum physics. Oftentimes we assume things natural from current knowledge to fit within a paradigm of healing. If this was the only approach, new and innovative applications would never be developed. The latest trend in the development and what is commonly mistaken for proper applications of low level laser therapy, are the influx in approvals for topical heating devices (ILY).4 These devices have an associated low level laser component, with the removal of the collecting lens from a high powered laser, but are not low level lasers. The problem is that when you remove the collecting lens out of configuration it ceases to be a focused laser. This in essences is now just a concentrated heat lamp, which gleans to the understanding of why market clearance was so easily obtainable. By far one the most difficult concepts of laser is the energy density or fluency, this component is what in large part relates to a non linear approach to understanding the applications. In the market place it is the focal point of sales in the approach that depth of penetration is somehow related to this component. Let’s look at common myths in laser therapy pertaining to power and how it correlates to penetration. Several articles have claimed, in this publication and other journals that you need more power to penetrate the tissue and that high power lasers are putting an end to low level lasers. The science of 3LT® has proven this to be untrue in many studies which will be referenced in this article. It is important to take into consideration that the FDA gave market clearance to the first high power therapeutic laser in 2004 (two years after the first low level laser); the approved device is manufactured by a company that filed substantial equivalence from a heat lamp (ILY) and in turn was given approval for topical heating and muscle relaxation not depth of penetration like the manufacturer claim. To date there have been no other 510(k) market clearances granted to any other “high powered laser” based on their own clinical trial. Low level lasers have endeavored in more substantial clinical, cellular & molecule trails that have not only been expensive to undertake, but time consuming; this is in part the reason why there are still very few indications for low power lasers. The companies marketing these high powered laser devices proclaim that they have more power and penetrate deeper than 3LT® devices (NHN). There is no research that proves these devices are more effective than a $600 heat lamp, not to mention they have the exact same marketing claims and can cost up to $50,000. There is also a question to the long term safety of these devices which has not been proven otherwise according to published research available. In evaluating the reference material of high powered lasers, almost every study referenced has been done with low level, low energy lasers, not high powered devices. New research published in Lasers in Surgery and Medicine in January 20065 states that “with as little as 10 joules you can cause damage to the DNA of the cell and decrease cell viability”. The laser used in the aforementioned study was a 3mW laser with a divergent beam and this article also stated “that since the laser used was a 3mW divergent beam it is not as harmful as a narrow parallel beam.” The research proves that even a low level laser can potentially cause damage if over treated; it would take only 1 second at 10 watts to over-stimulate to a level that can cause damage. Another myth is that high power lasers have biostimulation effects. Tiina Karu’s new text titled, Ten Lectures on Basic Science of Laser Phototherapy, highlighted a study by Rochkind et al (1988), were it was found that 540nm and 632.8nm had a strong effect on the action potential of the nerve and 904nm, as well as CW radiation at 660nm, 830nm, 880nm and 950nm had no effect.6 Since these wavelengths are not affecting the nerve through biostimulation they try and affect the nerve through heat which has a completely different consequence. In a statement made in Jan Tunér and Lars Hode Jan. 2008 2002 Laser Therapy book, “biostimulation based on current clinical research is .5 to 1 J/cm2 on an open wound and 2-4 J/cm2 through overlaying skin.”7 For a patient to receive the 00maximum of 4 joules required for biostimulation they would only need to treat the patient for 1 second with a 4 watt laser and 0.5 seconds with a 10 watt laser. This is in agreement with the Arndt-Schulz Law which states “weak stimuli excite biologic activity and strong stimuli retard this activity.”8 High powered lasers are used for tissue ablation, hair removal, acne, etc. The companies that produce these high powered lasers remove the collecting lens on these devices to prevent the device from burning the skin. In addition they have to manually scan (back and forth) the patient with these devices to keep from burning the tissue. The mechanism in which they are heating the skin proves that they are not penetrating deeper; according to Tunér and Hode article, Confounders and magicians3 where they state “because 980nm has a lower penetration capacity, more energy is absorbed in the upper part of the skin and the risk for overheating is greater.” They also state anything over “1 watt is excessive” in laser therapy.7 An additional article available in this publication titled Basic Principles of Low level Laser Therapy9 stated “super pulsing allows for deeper penetration,” the laser they were referencing was a 10 to 100 watt laser used at relatively low power which is conflicting with laser classifications due to the fact that it references a class IV laser which is not considered low power. These Class IV lasers are the same lasers used for resurfacing and tissue ablation without the focusing lens and the reason they super pulse them is because they are targeting a specific chromophore on the surface of the skin in which research has proven to be a topical treatment, that if left on the skin it would burn or ablate the subject. The author goes on to state “that it is well suited for medium and deep tissue, such as joints and tendons,” but offers no research or references. Let’s look at the research. Every laser has a plateau where it reaches bio-inhibition (Farok Al-Watban has published this in several wound studies)or it reaches a point where the application of laser is no longer effecting the physiological structures that are targeted. This concept is well published and we have already talked about biostimulation and its peek. In review of the published research we observe results for different power outputs, the indications of such devices and the consequences of excessive use. There are numerous studies and clinical results that compare different power outputs using the same wavelength only manipulating the time treated which is measured in J/ cm2 . The first example published in Photomedicine and Laser Surgery 200610 is a study using 685nm and 830nm laser on tissue repair in tendons on mice. In this study they used difference fluences and divided them in 6 groups, 2 placebo groups, 2 groups of 685nm laser (red) at 3 joules and 10 joules and 2 groups of 830nm (infrared) laser at 3 joules and 10 joules. Then they compared the results, the best results were with the 685nm at 3 J/cm2 and the results with the greatest consequence to healing were with 830nm at 10 J/cm2 . This study lends support to the fact that higher power and longer wavelengths do not lead to better outcomes. Similar findings have been published since at least 1989, when Shiroto stated that “an increase in irradiation dose may decrease biostimulatory effects.”11 As mentioned previously the first FDA market clearance was for chronic neck and shoulder pain. The laser in this study was a 5mW 635nm line generated beam (Erchonia). The treatment time was a total of one, 4 minute treatment. The results showed a difference in pain by 64% decrease in all patients treated in comparison to the placebo group, along with increased muscle strength and range of motion. The second market clearance for carpal tunnel was using a 100mW 830nm laser (Microlight). In this study they treated the patient three times a week for five weeks with each treatment for 15 minutes and at the end of the study there was a difference in pain of 6.6% between real and placebo patients. (this information was taken from company submissions to the FDA). These studies illustrate that less laser Jan. 2008 energy produces more efficient results. These were biostimulation lasers not high powered lasers. There is no tangible information available with high powered lasers for a therapeutic indication. Another myth with laser therapy is depth of penetration which seems easily disproved from the studies already noted, in addition to a 2001 MRI study by Rodrigo Neira, M.D. published in the America Journal of Cosmetic Surgery.12 This study showed that an 8mW 635nm laser that was held 6 to 8 inches from the skin could emulsify deep fat (6cm) and break up the appearance of scar tissue. Dr. Rodrigo proved this by showing abdominal MRI at 0, 4 and 6 minutes on T-1 and T-2 weighted sequences. This was later confirmed in a 2004 study published by Robert Jackson, M.D. in the AJCS journal13. These results are a stark contrast to the article published in Dynamic Chiropractic titled Basic Principles of Low Level Laser Therapy where the author stated that “red light at 640nm has been shown to effect skin, so it might be effective in treating cuts, scars, trigger points and acupoints. Usual depth of penetration is less than 10mm.”8 The author offers no research and this contradicts what the FDA gave clearance for and the two aforementioned articles prove is nothing more than a theory from the author. There seem to be many self proclaimed experts in laser therapy and the problem is none of them actually do any research. Tunér and Hode confirmed this with the author of this article they like most other so called or self professed laser experts form opinions based on what they read and who they are working for and not based on their own clinical or cellular research which they themselves have accomplished. There are countless studies, too numerous to list all in this article, that mention secondary effects using low level laser that do not rely on power. The fact is that there are no studies supporting high powered lasers for biostimulation and most every doctor knows that if you are heating the skin you are creating free radicals which were proven in the ASLMS study in January 2006.4 I believe every doctor should own a laser and eventually will, but there is an excess of inaccurate information from manufacturers and self professed laser experts that until more companies and laser excerpts actually do research, these articles will continue to confuse the end user. You owe it to yourself before you invest in any piece of equipment to have the manufacturer provide you research that was done with the device you are looking to purchase. If they have no research or they hand you research done by others and claim they can do the same, look else where. Just today I was called asking to provide research to a state board from a doctor that needed help because the state was telling him his device was experimental. If I had no cellular or clinical trial research to support the device he would no longer be able to use his laser, this has happened at least a half dozen times. Another consideration is if the laser manufacturer does not have liability insurance and something goes wrong you are left by yourself and in our litigious society it is almost certain, someone is going to get sued. There is a reason low powered lasers are in a class by themselves (NHN), they have proven results. Steven Shanks has been involved with 3LT® since 1996 and was responsible for the regulatory work involved and writing of the study for the first FDA 510(k) (NHN) in 2002. He has since accomplished three additional market clearances, submitted for a 4th and is working on 5 clinical trials. He works along with several universities and private practitioners to advance the field of 3LT® through clinical and cellular research. Jan. 2008 References 1. Oschman JL. The Biological Basis of Low Level Laser Light Therapy (3LT®). Nature’s Own Research Association. 2006 2. Center for Device and Radiological Health. U.S. Food and Drug Administration. RadiationEmitting Product Code: NHN. Viewed 4 September 2007.
http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfPCD_rh/classification.cfm?PCD=NHN. 3. Tunér and Hode. Confounders and magicians. Viewed 4 September 2007. http://www.laser.nu/lllt/pdf/confounders.pdf . 4. Center for Device and Radiological Health. U.S. Food and Drug Administration. RadiationEmitting Product Code: ILY. Viewed 4 September 2007. http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfPCD/classification.cfm?ID=4115 5. Hawkins DH and Abrahamse H. The role of laser fluence in cell viability, proliferation, and membrane integrity of wounded human skin fibroblast following helium-neon laser irradiation. Lasers in Surgery and Medicine. 38: 74-83; 2006. 6. Karu T. Ten Lectures on Basic Science of Laser Phototherapy. Prima Books in Sweden AB. 277; 2007. 7. Tunér and Hode. Laser Therapy Clinical Practice and Scientific Background. Prima Books AB. 2002. 8. Dorland's Illustrated Medical Dictionary. Merck Source. . Arndt Schulz Law. WB Saunders, an Elsevier imprint 2004. Viewed 4 September 2007. http://www.mercksource.com. 9. Kneebone WJ. Dynamic Chiropractic: Basic Principles of Low-Level Laser Therapy and Clinical Applications for Pain Relief. Viewed 4 September 2007. August 27, 2007, Volume 25 Issue 18. http://www.chiroweb.com/archives/25/18/04.html. 10. Carrinho PM, et al. Comparative Study Using 685nm and 830nm Lasers in the Tissue Repair of Tenotomized Tendons in the Mouse. Photomedicine and Laser Surgery. 24:6; 754-758; 2006. 11. Pontinen PJ. Low Level Laser Therapy as a Medical Treatment Modality. Urpo LTD. 2002. 12. Neira, R, et al. Low-Level Laser-Assisted Lipoplasty Appearance of Fat Demonstrated by MRI on Abdominal Tissue. The American Journal of Cosmetic Surgery. 18:3; 133-140; 2001. 13. Jackson RF, et al. Low-Level Laser-Assisted Liposuction. The American Journal of Cosmetic Surgery. 21:4; 191-198; 2004. your text here...
Harnessing low level laser therapy for revolutionary health solutions.
© 2025. All rights reserved.
On Point Health
202 E. Harcourt Rd. Suite 302
Angola, IN 46737
(260) 268-0099
administration@onpointhealth.care
© On Point Health. All rights reserved.
The information on this website is for educational purposes only and is not intended as medical advice, diagnosis, or treatment. Results may vary.
By using this website, you agree to our Privacy Policy Terms & Conditions.
By providing your phone number or email address, you consent to receive communications from On Point Health, including appointment reminders and relevant updates. Message frequency may vary. Message and data rates may apply. You may opt out at any time by replying STOP or using the unsubscribe link.
On Point Health respects your privacy and does not sell or share personal information. No mobile information will be shared with third parties/affiliates for marketing/promotional purposes. All the above categories exclude text messaging originator opt-in data and consent; this information will not be shared with any third parties.
📞 (260) 268-0099
🌐 www.onpointhealth.care
Send us an email with the link below.